New Allies Against Parkinson’s: Adaptive DBS & Subcutaneous Foslevodopa
June 26, 2025
We recently hosted an insightful webinar featuring Dr Alfonso Fasano, a leading neurologist specialising in movement disorders, who splits his time between Milan’s Humanitas Research Hospital and the University of Toronto. He introduced two innovative treatments that hold real promise for people living with Parkinson’s Disease (PD): Adaptive Deep Brain Stimulation (aDBS) and subcutaneous Foslevodopa.
1. Adaptive Deep Brain Stimulation (aDBS): A Smarter “Brain Pacemaker” 🧠
What it does:
Like traditional DBS, aDBS involves electrodes surgically implanted deep in the brain, connected to a battery-powered device under the skin.
Unlike standard DBS, which delivers continuous electrical stimulation, adaptive DBS adjusts itself in real time. The system “listens” to your brain activity and only activates precisely when needed—kind of like switching on the heating exactly when it gets cold rather than running it constantly.
Why it matters:
Conventional DBS has been transformative for many—helping with movement, rigidity, tremor—but side effects like speech troubles and stiffness can still occur.
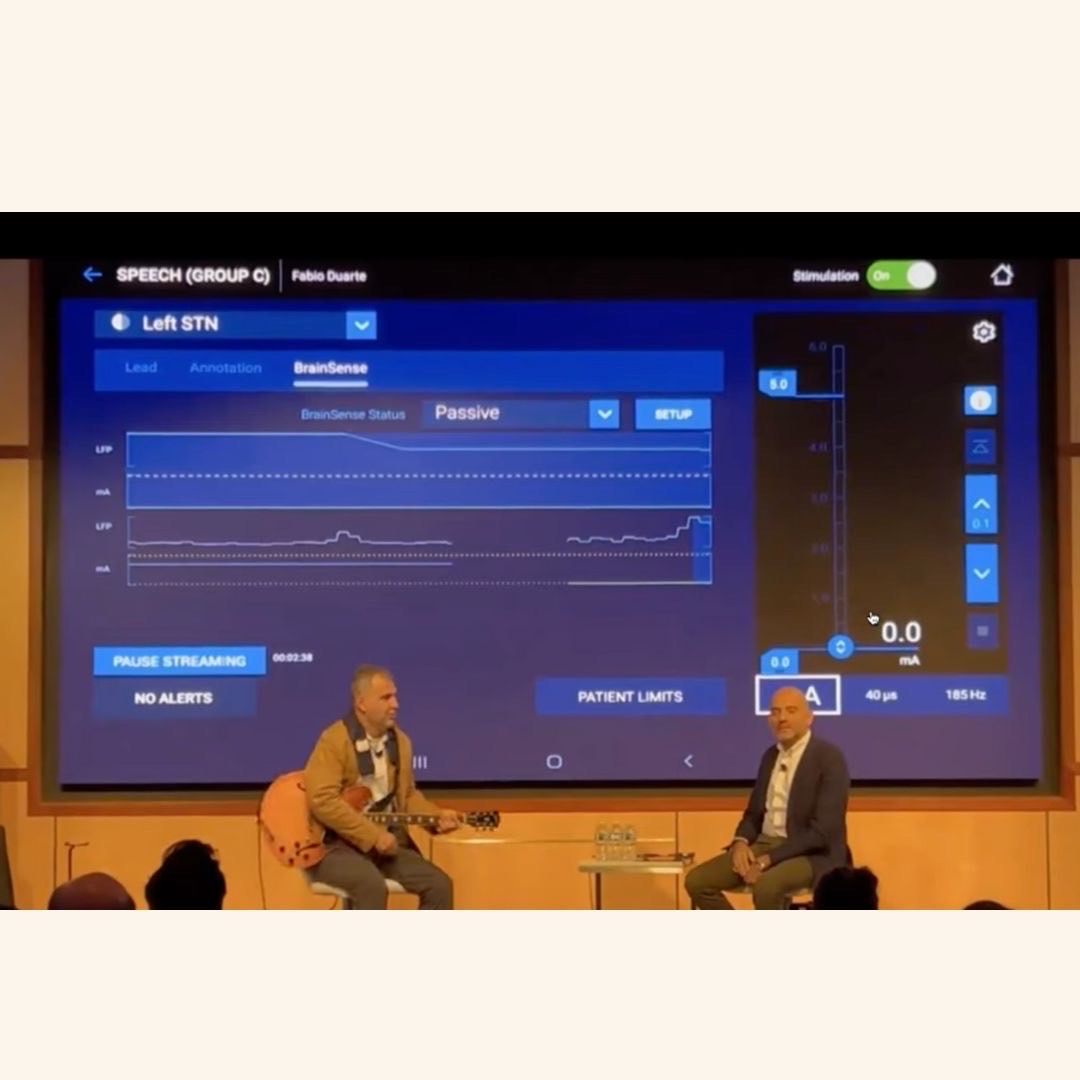
aDBS minimises overstimulation and improves symptom control, leading to better speech and reduced rigidity. Dr Fasano showcased a moving example: a guitarist whose tremor disappeared mid-performance once aDBS kicked in—yet his voice remained clear, unlike with standard stimulation.
The big picture:
Around the world, DBS is becoming more common; the introduction of aDBS represents the next major enhancement.
Behind this isn’t just tech—it’s about deep trust between patient and doctor, Dr Fasano emphasised. He even co-wrote a book with one of his aDBS patients, Benjamin Ster, reminding us that human connection matters as much as cutting-edge science.
2. Subcutaneous Foslevodopa: Smoother Dopamine Delivery
The challenge:
Oral levodopa is the gold standard treatment for PD—but patients often experience “on-off” periods as levels fluctuate, causing mobility from near-normal to stiff and slow.
The innovation:
Subcutaneous Foslevodopa uses a small pump to deliver levodopa smoothly under the skin, around the clock—24/7. This steady infusion dramatically reduces the peaks and troughs.
How it works:
A tiny tube (cannula) is inserted under your skin—abdomen, thigh or arm—and is changed every three days.
A portable pump carries doses equivalent to over 40 standard levodopa tablets over a full day!
No need for invasive procedures like feeding tubes or brain surgery.
Real-life gains:
Patients report better sleep—Parkinson’s “off” periods don’t always respect bedtime.
Motor symptoms ease: one man regained full neck flexibility and could tie his own shoes for the first time in years.
Even balance appeared to improve compared to those receiving standard or DBS therapy.
The caveats:
Skin irritation and infections are possible around the pump site. Switching cannulas every two days or finding new insertion spots can help.
Often, you’ll need specialised follow-up—at the start, frequent check‑ins are essential.
3. What About Radio Surgery (Focused Ultrasound)?
Dr Fasano also touched on MRI-guided focused ultrasound—a non-invasive “lesioning” technique aimed at specific brain regions to reduce tremor. It’s irreversible but may suit those not wanting implanted hardware.
4. Making the Right Choice: One Size Doesn’t Fit All
Choosing the best treatment depends on each individual:
4. Choosing What’s Right for You
Not all treatments are right for everyone. Dr Fasano gave some general pointers:
If your main symptom is tremor, aDBS or ultrasound may help most.
If your biggest issue is mobility at night, the continuous levodopa pump could be the answer.
If you struggle with speech or balance, aDBS is better than traditional DBS, which can sometimes worsen these.
If you prefer to avoid brain surgery, the pump is a good first step—leaving options open for DBS later.
And if you’re just unsure, it’s okay. The most important thing is talking it through with a doctor who respects your values and helps you understand your options.
Even though nearly half of people with Parkinson’s might benefit from advanced treatments like these, only about 15% currently go ahead—often because they’re not told about them, or don’t get the support to make an informed decision.
Real-world uptake shows that while around 45% of PD patients may be eligible for device-aided treatment, only about 15% go ahead—often due to fear, uncertainty or simply not having the information or support to decide. Dr Fasano emphasises the need for joint decision-making, with doctors guiding gently, not dictating, and fully respecting patient values and concerns.
5. The Future of Parkinson’s Care
aDBS is already being trialled in the UK’s NHS and is shedding new light on how to improve speech and reduce side effects.
Subcutaneous Foslevodopa is approved in some countries (it’s sold under brand names such as VioTH or Broodopa), and similar options from other companies are entering trials.
Advances in AI‑driven therapies, wearable monitoring, and personalised treatment plans are bringing us closer to a world where Parkinson’s care is precise, responsive, and patient-centred.
Final Thoughts
Both adaptive DBS and continuous levodopa infusion offer powerful, real-world benefits—less tremor, clearer speech, better sleep, and smoother daily living.
These aren’t just fancy gadgets; they’re carefully tailored solutions that integrate technology, neuroscience, and exceptional patient–doctor partnerships.
As this new generation of Parkinson’s care matures, the importance of informed choice and individual values will only grow—ensuring people with Parkinson’s co-pilot their own future, empowered and supported.
If you’d like a relatable recording of Dr Fasano in action or more background on any treatment, our webinar is archived in full, and we’re always here to help you understand what might suit you best.
Comments (0)
Loading comments...