Stem Cell Therapies for Parkinson’s: Dr. Gilbert Hosts - Are We Finally on the Verge of a Breakthrough?
January 17, 2026
 mister green
mister greenThe concept of using stem cells to treat Parkinson’s has always made perfect logical sense. If the condition is caused by the loss of specific dopamine-producing nerves in the brain, surely the best solution is to simply manufacture new nerves and replace them. For decades, this idea remained a distant hope, stuck in the laboratory or limited to small, experimental procedures. However, recent discussions between leading global experts suggest we have moved past the theoretical stage and are now seeing tangible, functional results in human trials.
In a recent update hosted by the APDA, Dr Jun Takahashi from Kyoto University and Dr Claire Hencliffe from the University of California, Irvine, shared data that suggests the field is maturing rapidly. We are no longer just asking if these cells can survive in a dish; we are seeing evidence that they can survive, grow, and function inside the human brain.
The Two Roads to Replacement
Current research is largely split into two approaches regarding where these new cells come from. Dr Takahashi, a pioneer in the field, focuses on Induced Pluripotent Stem Cells (iPS cells). This technology essentially acts as a biological time machine. Scientists can take a standard blood or skin cell from a donor (or potentially the individual themselves), ‘rewind’ it back into a stem cell, and then program it to become a dopamine neuron.
Dr Hencliffe discussed a different approach using Embryonic Stem Cells (ES cells), specifically a therapy known as bemdaneprocel. In this method, the cells are derived from established cell lines that have been grown in laboratories for decades. These 'juvenile' cells are transplanted into the brain with the expectation that they will mature and integrate into the existing network.
Safety First, Function Second
For years, the biggest fear surrounding stem cell therapy was safety. The worry was that injecting cells that are designed to grow might lead them to grow uncontrollably, potentially causing tumours. The data presented by both experts provides a significant sigh of relief. Dr Takahashi’s trial in Kyoto followed seven participants over two years. They found no evidence of tumour formation and no severe adverse events related to the cells. Similarly, the US-based trials discussed by Dr Hencliffe have shown a strong safety profile over three years.
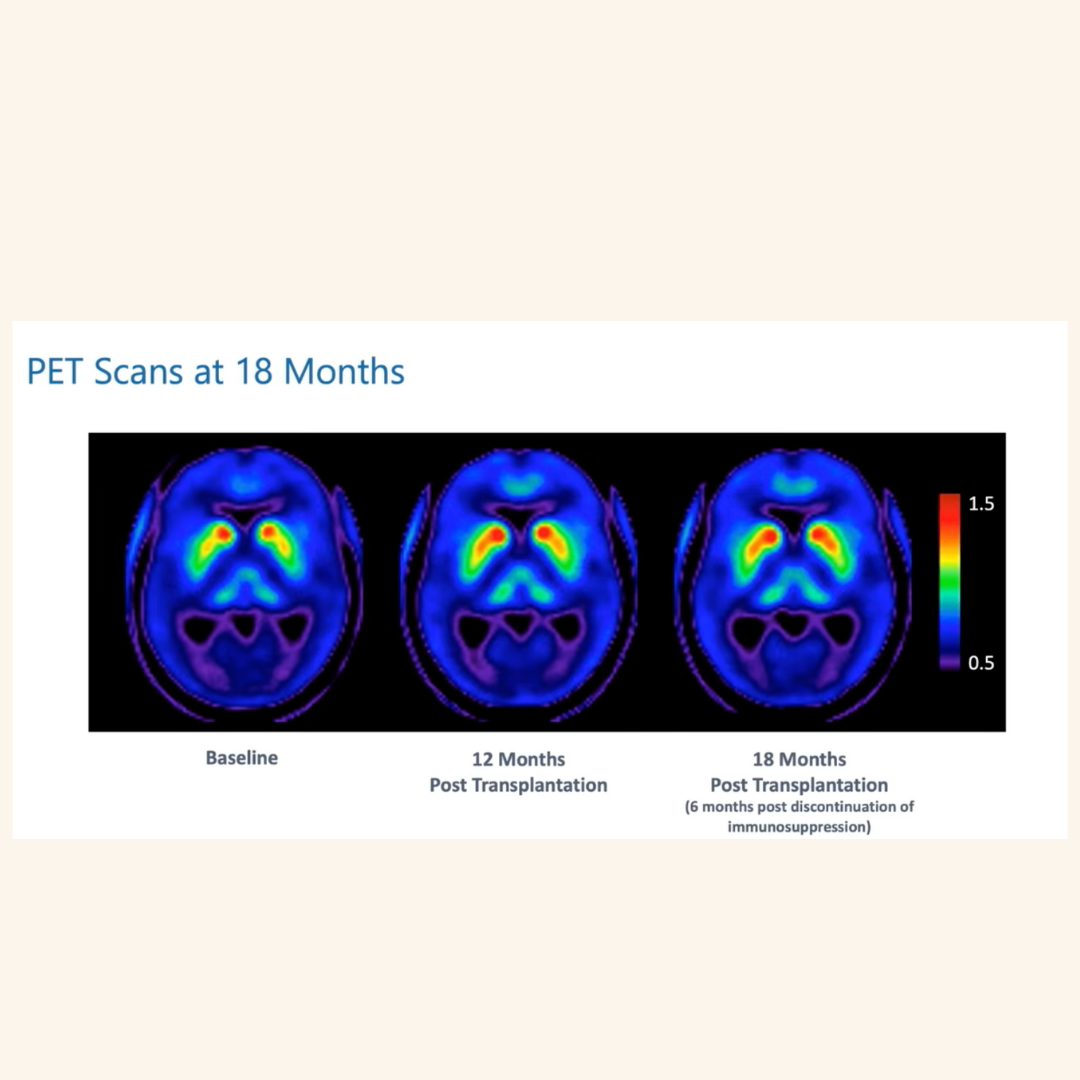
Beyond safety, the question remains: do they actually work? We cannot simply open a person’s skull to check if the cells are alive, so researchers use specialised PET scans. The images shared during the discussion were striking. They showed that the transplanted cells not only survived but began to light up the scan, indicating they were actively producing dopamine.
In terms of symptoms, the results are cautiously encouraging. In the Japanese trial, several participants saw an improvement in their 'off' time—the periods when oral medication wears off—with their motor function improving even when they were not taking medication. The US trial showed that those who received a higher dose of cells saw a greater reduction in their symptom severity compared to the low-dose group.
Who is This For?
As these therapies move closer to regulatory approval—with the bemdaneprocel trial notably skipping Phase 2 to move straight into a large Phase 3 trial—the question of eligibility becomes practical. Currently, these trials are designed specifically for idiopathic Parkinson’s. They are unlikely to be effective for 'Parkinsonisms' like MSA or PSP, as those conditions involve more widespread damage than just the loss of dopamine cells.
There is also the question of existing therapies. At the moment, individuals who have already undergone Deep Brain Stimulation (DBS) are generally excluded from these trials, although Dr Hencliffe noted that this might change in the future. The experts also highlighted that while the initial trials focused on people with established Parkinson's, the ideal candidates in the future might be those with Young Onset Parkinson's. For a younger person facing decades of managing the condition, a restorative therapy that repairs the brain's circuitry could offer a life-changing alternative to a lifetime of oral medication.
The Road Ahead
It is important to manage expectations. This is not a cure that stops the disease entirely, but rather a potential 'reset' of the motor symptoms. The transplanted cells replace the lost dopamine factory, but they do not necessarily stop the underlying biological processes that cause Parkinson's. However, the move from small safety studies to large-scale Phase 3 trials signals that stem cell therapy is graduating from experimental science to potential medical reality. The sheer amount of global collaboration, with trials now active across the US, Europe, and Asia, suggests that we are witnessing the beginning of a new chapter in how we treat the condition.
Comments (0)
Loading comments...